
Setting initial research directions for the core research theme of the Midlands PSRC
By Dr. Justin Aunger, PSRC Core Theme Research Fellow & Prof. Alice Turner, PSRC Co-Director
To celebrate the first year of the NIHR Midlands PSRC, we want to lay out some of our progress so far within the core theme. The Midlands PSRC has three themes including an Acute, Maternal, and Core Theme. The Core theme plans to conduct cross-cutting research that complements existing Acute and Maternal themes. This includes research into the organisational culture side of patient safety and into safety-critical issues in other clinical areas. In this blog, we explain the research areas we have investigated, those we have decided not to pursue, and what we are taking forward.
Investigating suggestions from the launch event
At the launch event of the PSRC, we collected ideas for important research avenues relating to patient safety and voted to reach a top 5. The top 5 ideas were as follows:
- How can we understand barriers and facilitators to clinical decision support tools used in maternity care?
- How do we measure if a team is safe?
- How do we develop a better shared understanding of patient perception of risk?
- How can patients contribute to safe acute care?
- What is the relationship between staff voice and safety outcomes/indices?
In the core team of the Midlands PSRC, we have been investigating the potential of these ideas and have decided to take some forward in different ways. “How do we measure if a team is safe” was identified as one of the most promising entries on this list. To investigate this, we performed a scoping review on this topic and identified that a lot of work has already been done around creation of tools for measuring safety in teams (Churruca et al., 2021; Ellis et al., 2023). We found that there is little agreement on the aspects which should be included in safety measures as these can include a wide range of items from leadership and leadership support, through available safety supporting systems, to adequacy of training. Similarly, it is difficult in modern care scenarios to determine what comprises a team. As such, we decided this is an important route for future research and one that is being explored by others, but is not a priority area for us as it stands.
Other entries we are pursuing in other ways, such as “How can patients contribute to safe acute care”. This is a core part of NHS Engand’s patient safety strategy for which, in 2021, they have published a “Framework for involving patients in patient safety” (NHS England, 2021). This includes implementing a new role across NHS Trusts, called Patient Safety Partners, which involves patients getting involved in organisational governance and management processes for patient safety. Another key programme is the rollout of Martha’s rule (Dyer, 2023). To enhance understanding in this area, we have published an advert for a self-funded PhD student to investigate this and other ways in which patients can improve the safety of their own care.
For number 5, “What is the relationship between staff voice and safety outcomes/indices?“, Dr. Justin Aunger and Prof. Russell Mannion (Core PSRC team members) are building upon their prior research with colleagues at Birmingham, Manchester, and Surrey, investigating ongoing activities to reduce unprofessional behaviours between healthcare staff in the NHS and the impact such behaviours can have on staff voice and patient safety.
Given the existing research in these areas and the routes we are already pursuing, we decided to also look to research avenues that fit within the clinical expertise of the PSRC team. A safety issue we identified was the proper follow-up of findings detected ‘accidentally’ during CT scans, often termed ‘incidentalomas’ (Chidiac and Aron, 1997). These incidental findings are often not communicated nor followed up properly (Litchfield et al., 2015; Barrett et al., 2022). A particular avenue aligned with the clinical expertise in the Midlands PSRC is to investigate the proper follow-up of small lumps (referred to as ‘pulmonary nodules’) in the lungs that can develop into lung cancer.
Identifying a new candidate for clinical decision-making support tools
Lung cancer is common and is most frequently diagnosed at a late stage, meaning on average, patients unfortunately have only a 10 percent chance of surviving for 10 years from diagnosis (Cancer Research UK, 2020). Therefore, it is important to do what we can to identify lung cancer cases early. Lung cancer screening, which is currently being rolled out across the UK, is one way we can try to catch it early.
Pulmonary nodules and lung cancer screening
Lung cancer screening is being offered to patients in the UK who are 55-74 years old who either smoke or used to smoke (Department of Health and Social Care, 2023). They will be booked an appointment to have a computed tomography (CT) scan of their lungs to identify cancer, but these scans often also identify smaller growths – called pulmonary nodules. Lung cancer screening populations, who are smoker and ex-smoker patients, have a high prevalence of nodules; data from the lung cancer screening trial show that, of 1994 participants who underwent CT screening, 1013 patients had nodules (50.9%) and 52 (2.6%) of the total number screened developed lung cancer (Marcus et al., 2019).
About 95% of all pulmonary nodules are benign, but a subset of these can become malignant (Mazzone and Lam, 2022). During screening, these scans can find growths which are large and potentially already a tumour (≥8mm diameter), medium sized and that need to be followed-up for a longer period of time (≥5mm diameter), or small enough to not be of any concern (<5mm diameter). Size is not the only malignancy-related characteristic of the nodules. There is also a type of nodule that is more diffuse and ‘sub-solid’ called ground glass nodules, and these too have an even greater chance of becoming cancer.
There are guidelines setting out how these nodules should be managed and followed-up. In the UK, these are the British Thoracic Society Guidelines, whereas in the USA, these are the Fleischner or American College of Chest Physician guidelines (Gould et al., 2013; Callister et al., 2015; MacMahon et al., 2017). In the British Thoracic Society Guidelines, larger nodules over 8mm in diameter are assessed via a method to estimate risk of malignancy called a ‘Brock model’, whereas medium-sized nodules of 5-8mm in diameter have their growth rate assessed by comparing baseline diameter to the diameter during a CT scan booked 3 months later (Figure 1). After this 3-month CT surveillance scan, the growth rate or ‘volume doubling time’ of the nodule will inform what steps are taken next (Mazzone and Lam, 2022). Steps taken can include discharge, further follow-up scans over 4 years, or biopsy. It is important the follow-up is performed correctly if lung cancer is to be caught early.
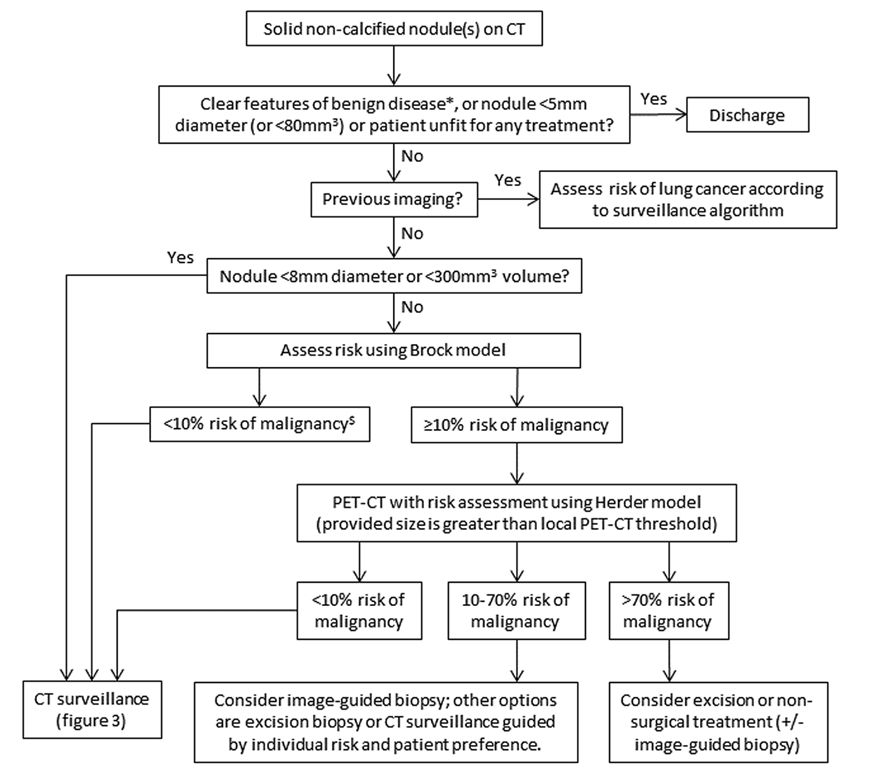
Figure 1. British Thoracic Society Guidelines for management of solid pulmonary nodules identified on CT scan.
Follow-up of incidentally-identified nodules in the NHS and abroad
The lung cancer screening programme has developed its own infrastructure for following up pulmonary nodules, and this is delivered by a private sector partnership with InHealth Group (Department of Health and Social Care, 2023). However, pulmonary nodules are also identified outside of the formal lung cancer screening programme. For example, nodules can be identified when the chest area is scanned for other reasons (such as when investigating heart problems). Up to 35 percent of the general population can have ‘incidental’ findings of pulmonary nodules when their thorax is CT scanned (Callister et al., 2015) and 50% of these have more than one nodule (Mazzone and Lam, 2022). Nodules found in this way are supposed to be reported by radiologists and referred to a respiratory clinician for follow-up. However, reportedly, the NHS does not have as robust an infrastructure for managing pulmonary nodule follow-up as the formal lung cancer screening programme. However, the UK is not alone in this – evidence from around the world suggests that these nodules are often followed up improperly even across very different health systems and contexts (Barrett et al., 2022; Schmid-Bindert et al., 2022; Mahboubian and King, 2023).
For example, in a retrospective cohort study across three hospitals in Canada, guideline adherence has been shown to be poor, with less than 50% of patients being followed up in a timely manner in line with guidelines (Kwan et al., 2019). A further retrospective observational cohort study in a large academic medical centre in the USA was able to quantify patient harm, by drawing on the medical records of 314 patients with incidentally identified nodules (Wayne, Prescott and Arenberg, 2022). Of these, the mean nodule size identified was 10.3 mm, 14.3% of nodules turned out to be malignant, and mean probability of cancer was 11.8%. Nodule management followed an evidence-based strategy in 245 patients (78.0%) and deviated in 69 patients (22%). Unfortunately, for patients who received non-guideline-adherent care, 14.49% of patients (10/69) received a delayed diagnosis of cancer. This compared to zero patients receiving guideline-adherent care (p<0.001) (Wayne, Prescott and Arenberg, 2022). Other studies have shown that guideline adherence is unfortunately worse for patients from underserved ethnic minority groups and those who are more socioeconomically deprived, which may exacerbate health inequalities (Schut and Mortani Barbosa, 2020).
In the UK, this issue is only recently gaining more attention. Currently, the only data available are from a recent week-long audit conducted at Royal United Hospitals Bath NHS Foundation Trust. There, the authors found that 15% of nodule cases received a ‘questionable’ clinical recommendation, which is equivalent to 1200 patients per year at this one hospital alone (Mahboubian and King, 2023). Improper follow-up of patients can occur for many reasons including improper recording/coding of findings against guidelines, errors in scheduling of follow-up, communication issues between care teams, or patient-side failures to attend appointments (Schut and Mortani Barbosa, 2020). Given this, to avoid unnecessary patient harm, it is important that patients with these nodules are followed up according to clinical guidelines. Luckily, there is evidence from abroad (mostly the USA), that adherence to guidelines can be improved.
Interventions to improve follow-up of pulmonary nodules
In our scoping of the literature so far, we have found at least fifteen interventions from non-UK countries to improve clinician adherence to clinical guidelines and improve patient follow-up. These interventions are of several types. Examples include process-based approaches e.g. to improve communication between healthcare professionals (Kang et al., 2020) and clinical decision making support tools to improve respiratory clinician guideline adherence (Lu et al., 2016). This decision making support tool was found to increase adherence to the guidelines of incidental findings (from 133 of 268 patients [50%] to 92 of 141 patients [65%], p = 0.003) (Lu et al., 2016). There are also automated technological systems to keep track of patients throughout their follow-up process (Shelver et al., 2017). An evaluation of this automated lung nodule registry tracking system found a significant decrease in tracking failure or delay when compared against published guidelines from 74% to 10% (p<0.001) across eight hospitals (Shelver et al., 2017). There are also.
Our research plan
Given the impact on patient harm, informal evidence from UK-based clinicians highlighting issues with patient follow-up of nodules, and ability to improve this pathway shown abroad, we have decided that this is a promising research direction for the PSRC. Together with respiratory medicine colleagues, we are developing a multi-pronged research approach comprising of three projects (Figure 2):
- To first establish the extent of deviation from follow-up, it will be necessary to develop a means for identifying patients who have nodules, as this may not be properly recorded in their clinical record. Our first project will be to develop a means for identifying patients with nodules based on their CT scan reports and what the radiologist recorded therein. We have been awarded £20k funding from the Institute for Interdisciplinary Data Science and AI at the University of Birmingham to fund data access to CT scan reports from University Hospitals Birmingham (UHB) that we can then use to develop a natural language processing (NLP) algorithm that reliably identifies nodule patients and classifies them according to nodule characteristics. NLP has previously been used successfully for identifying nodule patients in the USA (Basilio et al., 2023). Once patients are identified, we will then be able to retroactively identify if patients have been followed up correctly in line with guidelines. We will also be able to identify if there are inequities in terms of which patients are followed up with use of patient demographic data. We aim to start at UHB to identify patients to assess follow-up locally, before applying for further funding to look at the issue nationally with a much larger group of patients using the NLP algorithms we have developed.
- Our second project running parallel to this will be qualitative in nature and will explore, from the perspective of clinical and administrative staff at UHB, how deviations from guidelines may happen. It will also explore, with patients, their experience of moving through this care pathway. This will help to elucidate potential solutions.
- Our third project is to work, also in parallel, on a systematic review and meta-analysis of interventions to improve follow-up of patients and adherence to clinical guidelines for the management of incidentally identified pulmonary nodules worldwide. This would, along with the projects above, enable us to understand which intervention types are most effective. We also plan to perform a smaller scoping review to understand if other interventions have been used to improve follow-up of other incidental findings or ‘incidentalomas’. These would inform co-development of an appropriate intervention. An example intervention may be to develop a clinical decision-making support tool, depending on where the key issues in the pathway are identified and what types of interventions are most effective (Figure 2).
We are continuing to involve members of our patient and the public engagement group in our plans and will also keep you updated in future SafetyNET newsletters.
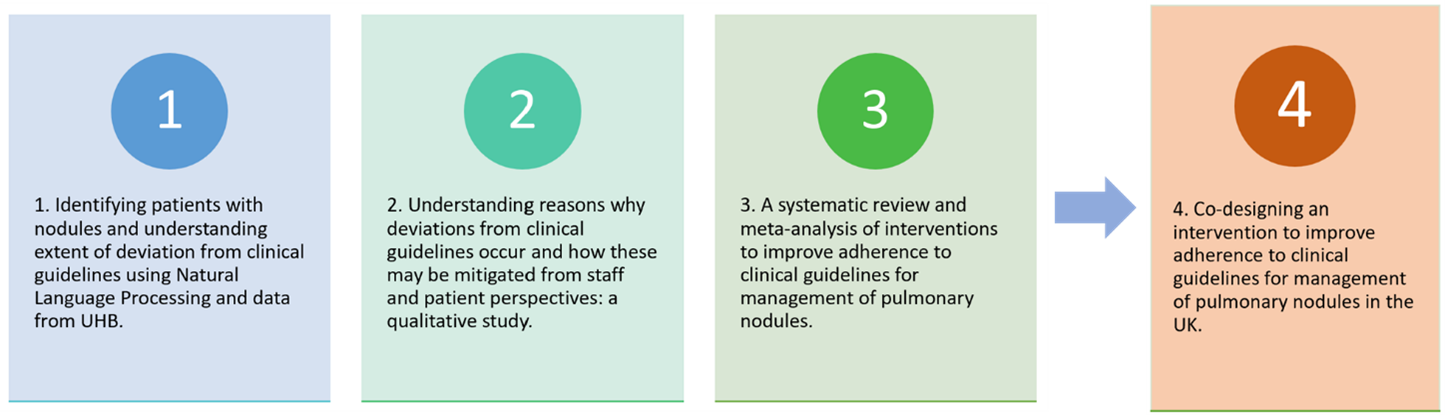
Figure 2. Depiction of our research plan to investigate adherence to clinical guidelines for management of pulmonary nodules.
Summary
Our Core theme team at the Midlands PSRC is pursuing a range of research avenues around organisational culture including patient involvement in their own safety, the impact of unprofessional behaviours between staff on patient safety and how this can be reduced, as well as novel research into improving the follow-up pathway of pulmonary nodules to reduce unnecessary patient harm in lung cancer.
We hope these research plans sound robust and promising. We would welcome any thoughts to Justin Aunger, research fellow in the core theme of the Midlands PSRC at j.aunger@bham.ac.uk.
References
Barrett, T.W. et al. (2022) ‘Catching Those Who Fall Through the Cracks: Integrating a Follow-Up Process for Emergency Department Patients with Incidental Radiologic Findings’, Annals of Emergency Medicine, 80(3), pp. 235–242. Available at: https://doi.org/10.1016/j.annemergmed.2022.04.026.
Basilio, R. et al. (2023) ‘Natural Language Processing for the Identification of Incidental Lung Nodules in Computed Tomography Reports: A Quality Control Tool’, JCO Global Oncology, (9), p. e2300191. Available at: https://doi.org/10.1200/GO.23.00191.
Callister, M. et al. (2015) ‘British Thoracic Society guidelines for the investigation and management of pulmonary nodules: accredited by NICE’, Thorax, 70(Suppl 2), pp. ii1–ii54.
Cancer Research UK (2020) ‘Lung cancer statistics’. Available at: https://crukcancerintelligence.shinyapps.io/EarlyDiagnosis/ (Accessed: 15 December 2023).
Chidiac, R.M. and Aron, D.C. (1997) ‘Incidentalomas: a disease of modern technology’, Endocrinology and Metabolism Clinics, 26(1), pp. 233–253.
Churruca, K. et al. (2021) ‘Dimensions of safety culture: a systematic review of quantitative, qualitative and mixed methods for assessing safety culture in hospitals’, BMJ Open, 11(7), p. e043982. Available at: https://doi.org/10.1136/bmjopen-2020-043982.
Department of Health and Social Care (2023) ‘New lung cancer screening roll out to detect cancer sooner’, 26 June. Available at: https://www.gov.uk/government/news/new-lung-cancer-screening-roll-out-to-detect-cancer-sooner (Accessed: 13 December 2023).
Dyer, C. (2023) ‘Martha’s rule: What could the proposed changes mean for doctors?’, BMJ, 382, p. p2067. Available at: https://doi.org/10.1136/bmj.p2067.
Ellis, L.A. et al. (2023) ‘Issues and complexities in safety culture assessment in healthcare’, Frontiers in Public Health, 11, p. 1217542. Available at: https://doi.org/10.3389/fpubh.2023.1217542.
Gould, M.K. et al. (2013) ‘Evaluation of Individuals With Pulmonary Nodules: When Is It Lung Cancer?’, Chest, 143(5), pp. e93S-e120S. Available at: https://doi.org/10.1378/chest.12-2351.
Kang, S.K. et al. (2020) ‘Process Improvement for Communication and Follow-up of Incidental Lung Nodules’, Journal of the American College of Radiology, 17(2), pp. 224–230. Available at: https://doi.org/10.1016/j.jacr.2019.11.023.
Kwan, J.L. et al. (2019) ‘Follow-Up of Incidental High-Risk Pulmonary Nodules on Computed Tomography Pulmonary Angiography at Care Transitions’, Journal of Hospital Medicine, 14(6), pp. 349–352. Available at: https://doi.org/10.12788/jhm.3128.
Litchfield, I. et al. (2015) ‘Test result communication in primary care: a survey of current practice’, BMJ Quality & Safety, 24(11), pp. 691–699. Available at: https://doi.org/10.1136/bmjqs-2014-003712.
Lu, M.T. et al. (2016) ‘Radiologist Point-of-Care Clinical Decision Support and Adherence to Guidelines for Incidental Lung Nodules’, Journal of the American College of Radiology, 13(2), pp. 156–162. Available at: https://doi.org/10.1016/j.jacr.2015.09.029.
MacMahon, H. et al. (2017) ‘Guidelines for management of incidental pulmonary nodules detected on CT images: from the Fleischner Society 2017’, Radiology, 284(1), pp. 228–243.
Mahboubian, A. and King, D. (2023) ‘Follow-up of indeterminate pulmonary nodules: Points of failure and AI-powered interventions’, 25 September. Available at: https://www.aidence.com/articles/follow-up-of-indeterminate-pulmonary-nodules/ (Accessed: 14 December 2023).
Marcus, M.W. et al. (2019) ‘Probability of cancer in lung nodules using sequential volumetric screening up to 12 months: the UKLS trial’, Thorax, 74(8), pp. 761–767. Available at: https://doi.org/10.1136/thoraxjnl-2018-212263.
Mazzone, P.J. and Lam, L. (2022) ‘Evaluating the Patient With a Pulmonary Nodule: A Review’, JAMA, 327(3), p. 264. Available at: https://doi.org/10.1001/jama.2021.24287.
NHS England (2021) Framework for involving patients in patient safety, pp. 1–69. Available at: https://www.england.nhs.uk/wp-content/uploads/2021/06/B0435-framework-for-involving-patients-in-patient-safety.pdf.
Schmid-Bindert, G. et al. (2022) ‘Incidental Pulmonary Nodules – What Do We Know in 2022’, Respiration, 101(11), pp. 1024–1034. Available at: https://doi.org/10.1159/000526818.
Schut, R.A. and Mortani Barbosa, E.J. (2020) ‘Racial/Ethnic Disparities in Follow-Up Adherence for Incidental Pulmonary Nodules: An Application of a Cascade-of-Care Framework’, Journal of the American College of Radiology, 17(11), pp. 1410–1419. Available at: https://doi.org/10.1016/j.jacr.2020.07.018.
Shelver, J. et al. (2017) ‘Effect of an Automated Tracking Registry on the Rate of Tracking Failure in Incidental Pulmonary Nodules’, Journal of the American College of Radiology, 14(6), pp. 773–777. Available at: https://doi.org/10.1016/j.jacr.2017.02.001.
Wayne, M.T., Prescott, H.C. and Arenberg, D.A. (2022) ‘Prevalence and consequences of non-adherence to an evidence-based approach for incidental pulmonary nodules’, PLOS ONE. Edited by M.-C. Lee, 17(9), p. e0274107. Available at: https://doi.org/10.1371/journal.pone.0274107.
Related
[related-posts-thumbnails]
PSRC network
NIHR Central London PSRC
NIHR Greater Manchester PSRC
NIHR Midlands PSRC
NIHR Newcastle PSRC
NIHR North West London PSRC
NIHR Yorkshire & Humber PSRC
Copyright © NIHR PSRC Network. All rights reserved.
Site hosted by The University of Manchester.
0 Comments
Trackbacks/Pingbacks